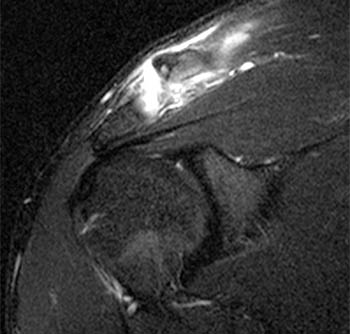
Clinical History: A 28 year-old male complains of shoulder pain after falling while playing ultimate Frisbee. A (1a) fat-suppressed T2-weighted coronal oblique image through the plane of the acromioclavicular joint and a (1b) fat-suppressed T2-weighted coronal oblique anterior to the plane of the acromioclavicular joint (ACJ) are provided. What are the findings? What is your diagnosis?
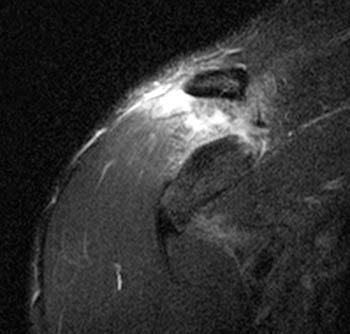
Figure 1:
A (1a) fat-suppressed T2-weighted coronal oblique image through the plane of the acromioclavicular joint and a (1b) fat-suppressed T2-weighted coronal oblique anterior to the plane of the acromioclavicular joint (ACJ)
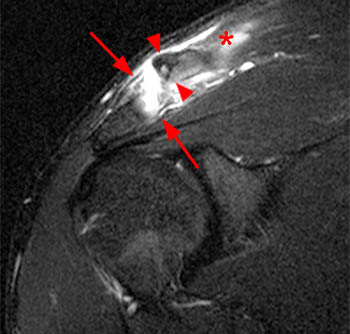
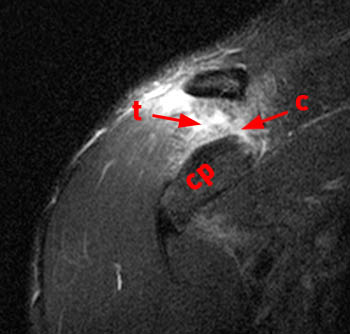
Figure 2:
(2a) The fat-suppressed T2-weighted coronal image demonstrates an acute injury of the ACJ with disruption of the superior and inferior acromioclavicular ligaments (arrows), widening of the ACJ and superior displacement of the clavicle (arrowheads) relative to the acromion. The trapezius muscle (asterisk) is partially torn. (2b) The corresponding fat-suppressed T2-weighted coronal image anterior to the plane of the ACJ demonstrates tears of the conoid (c) and trapezoid (t) ligaments which comprise the coracoclavicular ligamentous complex. cp: coracoid process.
Grade 3 acromioclavicular joint (ACJ) injury.
Injuries of the acromioclavicular joint (ACJ) are common, particularly in males involved in contact sports. The prototypical mechanism of injury to the ACJ involves a direct force produced when a patient falls on the shoulder with the arm adducted to the side. Although ACJ injuries occur with any contact sport, participants of hockey, rugby, and football are particularly vulnerable to ACJ injuries 1 . ACJ injuries account for approximately 10% of all shoulder injuries, occur five times more frequently in males, and occur most commonly in the second decade 2 .
The ACJ is a diarthrodial joint between the lateral surface of the clavicle and the medial surface of the acromion. Within the joint is a wedge-shaped fibrocartilaginous disk that projects into the joint from superior and inferior. The disk is not commonly visualized with routine MR imaging of the shoulder. The ACJ capsule is considered relatively weak with the strongest component at the superoposterior aspect, which is at the attachment site of the trapezius muscle 3 . The superior and inferior components of the acromioclavicular ligament complex reinforce the joint at small degrees of distraction 4 . With routine MR imaging, the ACJ capsule cannot be differentiated from the acromioclavicular ligaments, which insert into the capsule (3a). The trapezius and deltoid muscles are dynamic stabilizers and are particularly important when the ligamentous structures are torn. The trapezius has insertions sites at the superior aspects of the spine of the scapula and acromion. The deltoid muscle has sites of origin from the inferolateral spine of the scapula and acromion 5 . The superior acromioclavicular ligament blends into the aponeuroses of the deltoid and trapezius muscles 6 .
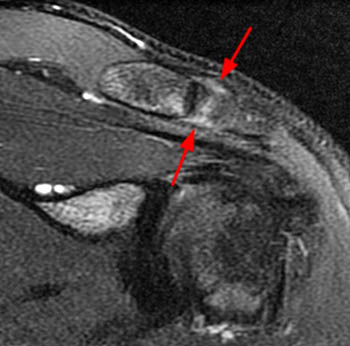
Figure 3:
A fat-suppressed T2-weighted coronal oblique image demonstrates the normal appearance of the superior and inferior acromioclavicular ligaments (arrows). The acromioclavicular ligaments cannot be differentiated from the ACJ capsule with routine MR imaging.
The coracoclavicular ligament complex is the main stabilizer of the ACJ, particularly at large degrees of separation 4 . The coracoclavicular ligament complex main function is that of vertical stabilization, which prevents superior and inferior translation of the clavicle 7 . The coracoclavicular ligament complex has two components, the conoid and trapezoid ligaments. The two ligaments anatomically form a V-shape and are separated by fat or a bursa 5 . In some patients, the fat separating the ligaments is sparse and the two components are confluent with one another (4a and 5a). The normal coracoclavicular ligaments are best visualized with T1 or proton density weighted images without fat suppression and can be visualized in the coronal and sagittal oblique planes.

Figure 4:
A T1-weighted coronal oblique image demonstrates the classic V shaped appearance of the trapezoid (t) and conoid (c) ligaments.

Figure 5:
In another patient, a coronal oblique T1- weighted image demonstrates a slightly different appearance of the ligaments. The trapezoid (t) and conoid (c) ligaments are more confluent in this variant.
The more medial component is the conoid ligament and is named for its triangular shape. The inferior apex of the conoid ligament is attached to the coracoid process. The conoid ligament spirals vertically and attaches to the conoid tubercle of the clavicle, which is at the junction of the lateral and middle thirds of the clavicle 5 . The conoid ligament’s main function is to prevent anterior and superior displacement of the clavicle 6 .
The more lateral component of the coracoclavicular ligament complex is the trapezoid ligament, named for its quadrilateral shape. The inferior segment of the trapezoid ligament is attached to the coracoid process and the superior segment is attached to the inferior aspect of the clavicle. The trapezoid ligament stabilizes against posterior clavicular displacement as well as providing resistance against anterior, superior, and inferior forces 5,6 .
With a direct force on the shoulder, the shoulder girdle and scapula are driven downward relative to the clavicle. When this happens, one of two injuries can occur: ACJ injury or clavicular fracture (or a combination of the two). Depending on the mechanism of injury, other directions of force can occur such as force in the anterior to posterior direction. ACJ injuries represent a continuum of ligament injuries. The mildest injury is a mild sprain of the AC ligaments. The next level of injury involves the coracoclavicular ligaments. The most severe level of injury involves injuries of the deltoid and trapezius muscular attachments. With more severe levels of injury, the upper extremity drops downward relative the distal clavicle and in extreme cases the skin overlying the AC joint can also be disrupted. In the rare situations, a severe direct force on the superior aspect of the distal clavicle with the arm in abduction will displace the clavicle inferiorly, below the level of the acromion or the coracoid 1 .
Although less common than direct force trauma, indirect forces may also cause ACJ injuries. A significant force can be transmitted to the AC joint via the humeral head from impaction injuries to the elbow or an outstretched hand. The humeral head impacts on the acromion and these injuries typically cause isolated ACJ injury without involvement of the coracoclavicular ligaments. These patients are also at higher risk for either fracture of the acromion or rotator cuff tear 8 . Uncommonly, a downward force produced by a pull mechanism while carrying a heavy load may cause an ACJ injury 1 .
Depending on the severity of the injury and patient’s body habitus, deformities of the ACJ may be seen on visual inspection. Palpation of the ACJ is performed to evaluate for deformities and areas of tenderness. If no luxation of the ACJ is present, reduction can be attempted by supporting the ipsilateral arm and applying a downward force on the distal clavicle to establish the type of ACJ injury 1 . In some situations, an abrasion is present over the superior aspect of the shoulder and can be seen at the site of impact. With more severe ACJ injuries, superior and inferior translation can be detected and this finding is called the “positive piano key sign” 9 . A shoulder shrug can be used to help differentiate between Grade 3 and 5 injuries shoulders. In a Grade 5 injury, the ACJ displacement is exaggerated in degree with the shoulder shrug 8 . Closed manipulation of the joint can help differentiate between Grade 3 and 5 injuries. If the deformity can be reduced, the deltotrapezial fascia is intact (Grade 3). If the deformity cannot be reduced, it suggests the deltotrapezial fascia is disrupted and the distal clavicle has buttonholed through the tear, preventing anatomic reduction (Grade 5) 8 .
Radiographic Evaluation
A routine radiographic series should be obtained on all patients with suspected ACJ injuries. Routine AP radiographs of the ACJ taken using a horizontal-beam technique may lead to superimposition of the ACJ on the spine of the scapula. The Zanca view uses a 10° to 15° cephalad angulation to better isolate the ACJ from other structures. Axillary projections can be performed to evaluate for anterior or posterior displacement of the distal clavicle 9 . Stress views of the ACJ are obtained using 10- to 15-lb of weight passively suspended from the upper extremity. Stress views are used to differentiate between Grade 2 and 3 injuries. Some authors have suggested that the usefulness of stress views do not outweigh the added cost, discomfort, and time 7 . The most important evaluation is the side-to-side comparison with the uninvolved side. It has been reported that an increase in the coracoclavicular distance of the injured shoulder over the asymptomatic contralateral shoulder by 25-50% represents complete coracoclavicular ligament disruption 10,11 .
CT imaging has no role in the routine evaluation of ACJ injuries. In certain circumstances, CT may add additional information if a complex fracture injury is also present that is not adequately defined with routine radiography.
At this time, MR imaging does not have a proven role in the routine evaluation of ACJ injuries. There is, however, no imaging modality that offers as much information regarding injuries to soft tissue structures. No other modality can directly image the coracoclavicular and acromioclavicular ligaments and muscle attachment sites of the deltoid and trapezius muscles. Osseous injuries are well evaluated with MR because of the inherent high sensitivity to fractures and also because the multiplanar images can display osseous displacement in relationship to adjacent structures.
The accuracy of MR imaging in staging of ACJ injuries has not been evaluated with Level I or Level II studies. Small published studies suggest that MR will detect injuries not suspected with routine clinical and radiographic staging. In a series of 13 patients, MR imaging results upgraded 20% of Grade 2 injuries and 50% of Grade 1 injuries 12 . In another small study of four patients, MR imaging showed disruption of the conoid and trapezoid ligaments in three patients with clinical Grade 2 and Grade 3 injuries. In a patient with a Grade 5 injury, only the trapezoid ligament was disrupted. The authors concluded that the clinical Rockwood classification did not correlate with the MR findings 13 . One report has indicated that MR can detect tears of the acromioclavicular ligaments 3 but other reports indicate that MR cannot reliably detect acromioclavicular ligament tears in Grade 1 ACJ injuries 5,12 .
The current orthopaedic literature is in general agreement that routine MR imaging for ACJ injuries is not indicated 8,9,14 . If the prevailing local practice is to treat Grade 3 injuries conservatively, then MR imaging would have a limited role in that community. If the prevailing local practice is to surgically treat Grade 3 injuries, then MR imaging could have a role in differentiating Grade 2 from Grade 3 injuries when radiographic and clinical findings are equivocal. The role of MR imaging is evolving and for the time being should be used in selective cases to guide appropriate therapy. Another advantage of MR imaging is the ability to evaluate adjacent structures that may be injured. For example, the rotator cuff complex, labral complex, humeral head and glenoid can all be examined for possible injuries.
The Rockwood classification for ACJ injuries is widely used in clinical practice. The classification system is unfortunately, in some respects, non-intuitive and non-linear. For example, Grade 1 through Grade 3 and then Grade 5 injuries represent a linear continuum of progressively more severe injuries whereas Grade 4 and 6 represent injuries that do not fit neatly into progression of the injuries. Logically, the classification should have two major categories: nonoperative ACJ injuries and operative ACJ injuries. Having said that, the following discussion is a review of the categories as they now exist.
Grade 1 injuries represent a sprain of the acromioclavicular ligament only without a complete tear (6a). The AC joint remains stable, and the ligaments are intact. ACJ tenderness is minimal to moderate without a palpable deformity (1). Radiographs are normal with and without weight bearing. As discussed earlier, it has been stated that MR imaging will show tears of the superior component of the acromioclavicular ligament in Grade 1 injuries 3 . Others have disagreed with this finding stating that no specific MR findings are seen with Grade 1 injuries, particularly in adults who commonly have pre-existing chronic findings that are indistinguishable from mild acute trauma 5 .